.png)
Types of Facial Pigmentation Explained: Your 2026 Guide
- chevonne stewart
- 2 days ago
- 8 min read


Facial pigmentation refers to changes in skin color caused by variations in melanin production, resulting in conditions like melasma, solar lentigines, and post-inflammatory hyperpigmentation (PIH). Melanin is the pigment produced by melanocytes, specialized cells in the skin’s basal layer. Two primary forms exist: eumelanin, which produces brown and black tones, and pheomelanin, which produces red and yellow tones. When melanocytes overproduce or underproduce melanin, visible discoloration appears on the skin. Understanding the types of facial pigmentation explained here gives you a clear foundation for recognizing your own skin and making informed choices about treatment.
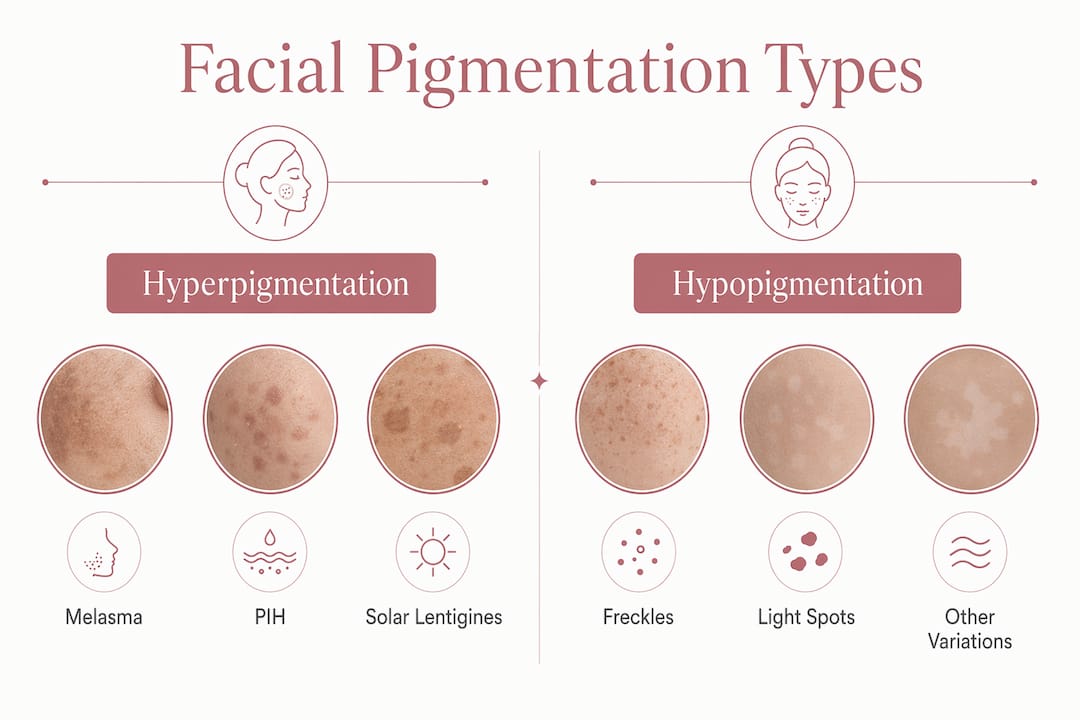
What are the main types of facial pigmentation?
Facial hyperpigmentation types fall into four major categories, each with distinct features, triggers, and treatment responses. Knowing which type you have is the first step toward choosing the right approach.
Melasma
Melasma presents symmetrically on sun-exposed areas of the face, including the cheeks, forehead, upper lip, nose, and chin. The patches appear brown or gray-brown and tend to deepen with sun exposure and hormonal changes. Melasma is more common in women, particularly during pregnancy or while using hormonal contraceptives. It does not resolve on its own and requires consistent management.

Solar lentigines (sun spots and age spots)
Solar lentigines are well-defined, round brown spots caused by cumulative sun exposure over years. They commonly appear on the face, hands, and décolletage. Unlike melasma, they are not symmetrical and do not fluctuate with hormones. They are a reliable marker of long-term UV damage.
Post-inflammatory hyperpigmentation (PIH)
PIH develops after skin trauma such as acne, burns, or injury, when the healing process triggers excess pigment production. It appears as flat, darkened patches at the site of the original inflammation. PIH is more pronounced in people with deeper skin tones. It can fade over time but often requires targeted treatment to resolve fully.
Freckles (ephelides) and hypopigmentation
Freckles are hereditary, UV-sensitive spots linked to MC1R gene variants, common in fair skin, and they darken in summer and fade in winter. Hypopigmentation, by contrast, describes areas where melanin is reduced or absent, resulting in lighter patches. Conditions like vitiligo and post-inflammatory hypopigmentation fall into this category. Both freckles and hypopigmentation signal that melanocyte activity is disrupted, though in opposite directions.
Type | Appearance | Primary trigger | Skin tone most affected |
Melasma | Symmetric gray-brown patches | Hormones, UV exposure | All tones, especially medium-dark |
Solar lentigines | Round, defined brown spots | Cumulative sun exposure | Fair to medium |
PIH | Flat dark patches at injury site | Inflammation, trauma | Deeper skin tones |
Freckles | Small, scattered brown spots | UV exposure, genetics | Fair skin |
Hypopigmentation | Light or white patches | Inflammation, autoimmune | All skin tones |
What causes facial pigmentation?
Facial pigmentation causes are rarely single-factor. UV radiation, hormones, inflammation, genetics, and even heat each play a role, and they often interact.
UV and visible light exposure are the most consistent triggers across all pigmentation types. UV rays stimulate melanocytes to produce more melanin as a protective response. What many people miss is that visible light, particularly high-energy visible (HEV) light from screens and sunlight, also activates melanin production. This is why standard UV-only sunscreens are insufficient for conditions like melasma. Tinted sunscreens containing iron oxides block both UV and visible light, making them a far more effective shield.
Hormonal influences are a major driver of melasma specifically. Estrogen and progesterone increase melanocyte sensitivity, which is why melasma often appears or worsens during pregnancy, when using oral contraceptives, or during hormone replacement therapy. This hormonal connection also explains why melasma is so much more common in women than in men.
Inflammation and skin trauma trigger PIH by activating melanocytes during the healing process. Acne, eczema, psoriasis, and even aggressive skincare treatments can all leave behind dark marks. People with Fitzpatrick skin types IV through VI (medium-brown to dark skin) are significantly more prone to PIH because their melanocytes are more reactive.
Genetic predisposition shapes baseline melanocyte activity and determines how your skin responds to external triggers. Freckles, for example, are directly linked to inherited MC1R gene variants. Your genetic skin phototype also influences how quickly pigmentation develops and how deeply it sets in.
UV and visible light stimulate excess melanin production
Hormonal changes increase melanocyte sensitivity, especially in melasma
Skin inflammation from acne, burns, or procedures triggers PIH
Genetic factors determine baseline melanocyte reactivity
Heat exposure can worsen existing pigmentation conditions
Pro Tip: Avoid hot showers, saunas, and intense heat exposure when managing active pigmentation. Heat activates melanocytes independently of UV, which means your skin can darken even on cloudy days spent indoors near a heat source.
How to treat facial pigmentation effectively
Treating facial pigmentation requires matching the approach to the specific type. A treatment that works well for solar lentigines may worsen melasma, so getting this right matters.
Daily broad-spectrum tinted sunscreen. Tinted sunscreens with iron oxides block both UV and visible light, which is the foundational step for every pigmentation type. Photoprotection prevents melanin memory, the process by which melanocytes “remember” past UV damage and respond more aggressively to future exposure. Apply every morning, regardless of weather or season.
Topical brightening agents. Ingredients like niacinamide, azelaic acid, kojic acid, and vitamin C inhibit tyrosinase, the enzyme that drives melanin production. These are appropriate first-line options for melasma, PIH, and solar lentigines. Consistency over weeks to months is required to see measurable results. For a deeper look at how natural actives treat pigmentation, botanical ingredients like licorice root and tranexamic acid are gaining strong clinical support.
Oral tranexamic acid combined with microneedling. This combination achieves a 50% reduction in pigmentation within 60 days, compared to 30% with topical triple combination cream alone. This makes it a significantly more effective option for moderate to severe melasma. Oral tranexamic acid works by blocking the signaling pathway that triggers melanocyte activity.
Professional chemical peels. Peels using acids like glycolic, lactic, or mandelic acid accelerate cell turnover and reduce surface pigmentation. They are particularly effective for superficial PIH and solar lentigines. Reviewing pigmentation treatment options compared can help you understand which peel depth suits your pigmentation type.
Lasers and light-based therapies. These are second-line treatments, best suited for stubborn solar lentigines and superficial pigmentation. Lasers and chemical peels can worsen pigmentation when applied to inflamed or unconditioned skin. Pre-treatment skin conditioning with topical agents for 4–8 weeks before any procedure significantly reduces the risk of PIH as a side effect.
Pro Tip: Never book a laser or peel treatment during a period of active skin inflammation, recent sun exposure, or hormonal fluctuation. Timing your treatment during a stable skin phase gives you the best chance of a positive outcome without triggering new pigmentation.
How can you identify your pigmentation type at home?
Recognizing your pigmentation type before seeking treatment saves time and prevents the wrong approach from making things worse. Several self-identification clues help narrow down what you are dealing with.
Symmetry: Melasma appears in matching patterns on both sides of the face. PIH and solar lentigines are typically asymmetric.
Location: Melasma favors the cheeks, forehead, and upper lip. Solar lentigines cluster on areas with the most sun history. PIH appears exactly where a breakout or injury occurred.
Color: Brown patches that shift to gray in certain lighting often indicate deeper, dermal melasma. Flat, uniform brown spots are more typical of solar lentigines.
Seasonal change: Freckles darken in summer and fade in winter. Melasma also worsens with sun exposure but does not fully fade in winter without treatment.
Trigger pattern: If your pigmentation appeared after a breakout, procedure, or skin injury, PIH is the most likely cause.
When pigmentation appears suddenly, changes shape, has irregular borders, or is accompanied by itching or bleeding, see a dermatologist promptly. These features can indicate conditions that require medical evaluation beyond cosmetic treatment. A dermatologist may use the Melasma Area and Severity Index (MASI) score to measure pigmentation extent and track treatment progress objectively. Over-the-counter products containing niacinamide, vitamin C, and azelaic acid are safe starting points for most pigmentation types while you await a professional consultation. Understanding how pigmentation forms under the skin also helps you set realistic expectations for how long treatment takes.
Key Takeaways
Treating facial pigmentation effectively requires identifying the specific type first, because melasma, PIH, solar lentigines, and hypopigmentation each respond to different interventions.
Point | Details |
Know your type | Melasma, PIH, solar lentigines, and hypopigmentation each have distinct triggers and treatments. |
Sunscreen is non-negotiable | Tinted broad-spectrum sunscreens with iron oxides block both UV and visible light to prevent recurrence. |
Combination therapy outperforms topicals | Oral tranexamic acid with microneedling achieves 50% pigmentation reduction vs. 30% with topical cream alone. |
Timing matters for procedures | Lasers and peels applied to inflamed or unconditioned skin can worsen pigmentation, especially PIH. |
Self-identification is possible | Symmetry, location, color, and trigger patterns help you distinguish between pigmentation types before consulting a professional. |
What 15 years of treating pigmentation has taught me
The most common misconception I see is that pigmentation can be “cured.” It cannot. Melasma in particular is a chronic condition that requires ongoing management, not a one-time fix. Clients who understand this from the start get better results because they stay consistent with their sunscreen, their maintenance treatments, and their lifestyle habits.
The second thing I have learned is that photoprotection compliance is the single biggest predictor of treatment success. I have seen clients invest in excellent professional treatments and then undo months of progress with a few unprotected days in the sun. Tinted sunscreen with iron oxides is not optional for anyone managing melasma or PIH. It is the treatment.
I am genuinely encouraged by the growing body of evidence behind oral tranexamic acid and combination protocols. These approaches are giving clients results that topical-only regimens simply cannot match. At the same time, I always pre-condition skin before any peel or device treatment. Skipping that step is the fastest way to trigger new PIH, especially in clients with deeper skin tones.
My practical advice for anyone managing pigmentation long term: treat your skin as a system, not a problem to be solved once. Consistent sun protection, targeted actives, and professional treatments timed to your skin’s stable phases will always outperform aggressive, reactive approaches. Healthy, confident skin is built over time, and that is worth understanding.
— chevonne
Personalized pigmentation treatments at Fundamentalskin
Fundamentalskin, led by Dermal Clinician Chevonne with 15 years of clinical experience, offers targeted treatments designed specifically for facial pigmentation concerns.
The Larimedical Biomimetic Peel addresses uneven skin tone and discoloration without downtime, making it a practical option for clients managing melasma, PIH, or sun damage. The Biomimetic Peel combined with LED Therapy takes this further by pairing chemical exfoliation with light therapy to support skin renewal and reduce pigmentation. The Synergie Peel is another option for clients seeking a targeted approach to surface discoloration. Every treatment at Fundamentalskin uses Australia-sourced, organic ingredients and is personalized to your skin’s specific needs. Book a consultation to find out which treatment is right for you.
FAQ
What is the difference between melasma and sun spots?
Melasma appears as symmetric gray-brown patches triggered by hormones and UV exposure, while solar lentigines are defined brown spots caused by cumulative sun damage. Melasma fluctuates with hormonal changes; sun spots do not.
Can facial pigmentation go away on its own?
PIH can fade gradually over months without treatment, but melasma and solar lentigines rarely resolve without targeted intervention. Consistent sun protection slows progression and supports any active treatment.
What is the best sunscreen for facial pigmentation?
Tinted broad-spectrum sunscreens containing iron oxides are the most effective choice because they block both UV and visible light, both of which trigger melanin production.
How long does it take to see results from pigmentation treatment?
Topical treatments typically show visible improvement after 8–12 weeks of consistent use. Combination protocols using oral tranexamic acid and microneedling can achieve measurable results within 60 days.
When should I see a professional about skin discoloration?
See a dermatologist or qualified clinician if pigmentation appears suddenly, changes shape, has irregular borders, or does not respond to over-the-counter products after 12 weeks of consistent use.
Recommended
Comments